Embryology, Gross Anatomy & Bronchi
The structural foundations that underpin every thoracic operation — from single-lung ventilation to segmentectomy.
Embryology
Lung development begins at week 3 to 4 of gestation. The respiratory epithelium derives from endoderm; connective tissue, cartilage, and muscle derive from splanchnic mesoderm and neural crest cells.
The lung bud (respiratory diverticulum) develops as an out-pouching of foregut endoderm by the late third or early fourth week. The proximal portion becomes the trachea; the distal bulbous end forms the bronchial buds, which give rise to all lower respiratory structures.
| # | Stage | Timeline | Key events |
|---|---|---|---|
| 1 | Embryonic | 0–5 weeks | Lung bud formation |
| 2 | Pseudoglandular | 5–16 weeks | Formation of major airways |
| 3 | Canalicular | 17–28 weeks | Peripheral airway division; epithelial differentiation; vascularisation; air-blood barrier formation |
| 4 | Saccular | 28 weeks – birth | Type I and II pneumocyte differentiation; surfactant production |
| 5 | Alveolar | 28 weeks – 8 years | Alveolar multiplication; extensive increase in surface area |
Gross anatomy

Lobes and fissures
2 fissures: oblique + horizontal
1 fissure: oblique only
Surface anatomy
The parietal pleura projects superiorly 1 inch (2.5 cm) above the midpoint of the medial third of the clavicle. Both pleural reflections cross the 8th rib at the mid-clavicular line, the 10th rib at the mid-axillary line, and reach the paraspinal region just below the 12th rib posteriorly. The lungs follow but extend two rib spaces less than the pleura below the 6th rib anteriorly.
The gap between lung margin and pleural reflection below the 6th rib anteriorly is the safe zone for thoracocentesis in the sitting patient. Intercostal drain insertion must respect these surface markings to avoid lung puncture.
Anatomical variations
- Horizontal fissure may be incomplete — partial or complete fusion of upper and middle lobes
- Superior segment of lower lobe may be delineated by a separate accessory fissure
- Accessory fissures and lobes may occur in one or both lungs
A normal variant of the apical segment of the right upper lobe — caused by failure of the azygos vein to migrate, creating a deep fissure invaginated by two layers of pleura. Not a true accessory lobe. Usually incidental on imaging but can cause technical difficulty during surgery.
Bronchi
The trachea bifurcates into right and left main bronchi at the level of T4. The carina (Latin: keel of a ship) is the sharp cartilaginous ridge at this division — the most sensitive area for triggering the cough reflex.
The right upper lobe bronchus takes off within 1–2 cm of the carina. A right-sided DLT or bronchial blocker advanced too far will obstruct the RUL. Always confirm position with a fibreoptic bronchoscope after placement and after repositioning.
Divisions of the right mainstem bronchus
Divisions of the left mainstem bronchus
The conducting zone and acinus
Bronchi undergo an average of 23 divisions. The first 16–17 generations form the conducting zone — anatomical dead space, no gas exchange. Beyond a terminal bronchiole lies the acinus — the gas-exchanging unit — comprising respiratory bronchioles, alveolar ducts, and alveoli.

Tracheal bronchus (pig bronchus / bronchus suis)
An ectopic bronchus arising from the right lateral wall of the trachea, typically within 2 cm of the carina, supplying segments or all of the right upper lobe. Incidence approximately 0.1–2%, clear right-sided predilection.
Supernumerary type: accessory bronchus alongside a normal RUL bronchus — normal segmental anatomy preserved.
Displaced type: replaces one or more segments of the upper lobe bronchus — most commonly the apical segment.
- Intubation risk: ETT or DLT advanced past the orifice may obstruct the tracheal bronchus, causing atelectasis of the supplied segment
- Lung isolation: bronchial blocker or DLT placement must account for anomalous anatomy — confirm bronchoscopically
- Recurrent infection: impaired drainage causes recurrent RUL pneumonia — an under-recognised cause
In any patient with recurrent right upper lobe infections or difficulty with lung isolation, look specifically for a tracheal bronchus on pre-operative CT before theatre.
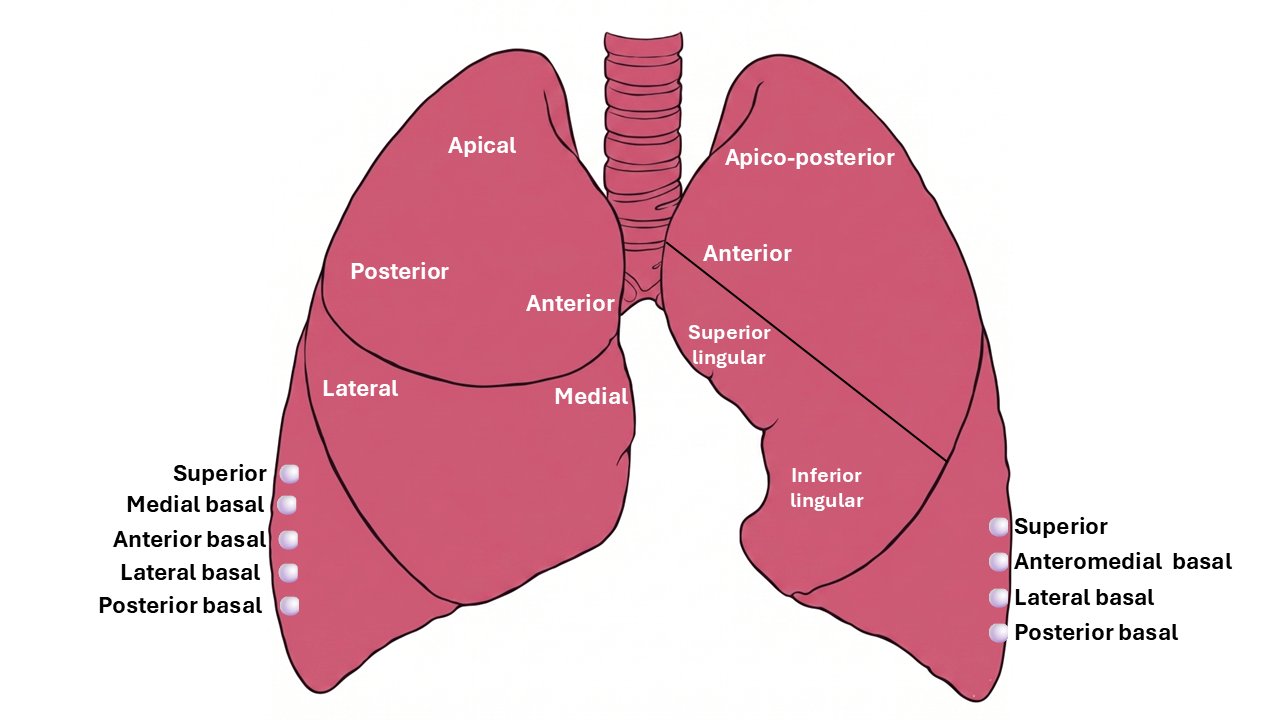
Bronchopulmonary segments
A bronchopulmonary segment (BPS) is an anatomical unit of lung supplied by a specific tertiary (segmental) bronchus with an accompanying segmental artery. The general pattern is 10 segments on the right and 8 segments on the left — LB1/2 and LB7/8 are typically fused on the left.
Pyramidal in shape — apex towards the root of the lung, base towards the surface. Each segment has its own arterial supply and segmental bronchus. Pulmonary veins run in intersegmental planes, not alongside bronchi — forming the surgical plane between adjacent segments.
Each BPS has no communication with adjacent segments — making segmentectomy possible without damaging neighbours. Intersegmental planes are marked by intersegmental veins, which serve as the surgical guide. There is little bleeding or air leak after segmentectomy if the intersegmental plane is correctly developed.
All clinical content should be verified against current guidelines before clinical application. This resource is intended for revision and educational purposes only.
Standard textbooks
- Shields TW, LoCicero J, Reed CE, Feins RH. General Thoracic Surgery. 7th ed. Lippincott Williams & Wilkins.
- Sellke FW, del Nido PJ, Swanson SJ. Sabiston & Spencer Surgery of the Chest. 9th ed. Elsevier.
- Pearson FG, et al. Thoracic Surgery. 3rd ed. Churchill Livingstone.